








 52 / 330
52 / 330

52
28
TH
CONGRESS OF THE ESPU
08:44–08:47
S4-6 (PP)
DUPLEX SYSTEMS: TOP-DOWN
OR BOTTOM-UP APPROACH?
David KEENE
1
and Ramnath SUBRAMANIAM
2
1) Royal Manchester Children’s Hospital, Department of Paediatric Urology, Manchester, UNITED KINGDOM - 2) Leeds
Teaching Hospitals NHS Trust, Department of Paediatric Urology, Leeds, UNITED KINGDOM
PURPOSE
To compare whether a top-down or bottom-up approach results in different likelihoods for further
surgery.
MATERIAL AND METHODS
A prospectively database was maintained for patients undergoing surgery for duplex systems by
a single surgeon between 2003 and 2015. Patients were classified into 2 groups; Group 1 initial
intention for upper approach (heminephroureterectomy-HN) or Group 2 lower approach (bladder
reconstructive surgery-BRS). The requirement for further surgery was recorded; endoscopic inci-
sion (EI), bladder reconstructive surgery (BRS), endoscopic correction of reflux (ECR), hemineph-
roureterectomy (HN). Indications for initial and subsequent surgery included urinary tract infection,
VUJ obstruction and incontinence. Endoscopic incision was not performed for patients with an
asymptomatic ureterocele. Fisher’s exact test with a 2-tail p value <0.05 was used.
RESULTS
79 patients underwent surgery for duplex systems. 39 patients had HN initially (Group 1) and
40 patients had BRS initially (Group 2).
Further surgery was performed in 28% of patients from Group 1 (8 BRS, 5 EI) vs 5% of patients from
Group 2 (1 redo BRS, 1 ECR). Significantly less additional surgical procedures were performed after
BRS compared to HN (p=0.006). The presence of either reflux or ureterocele increases the chances
of further surgery in those patients who had HN initially compared to BRS (p=0.02, p=0.002).
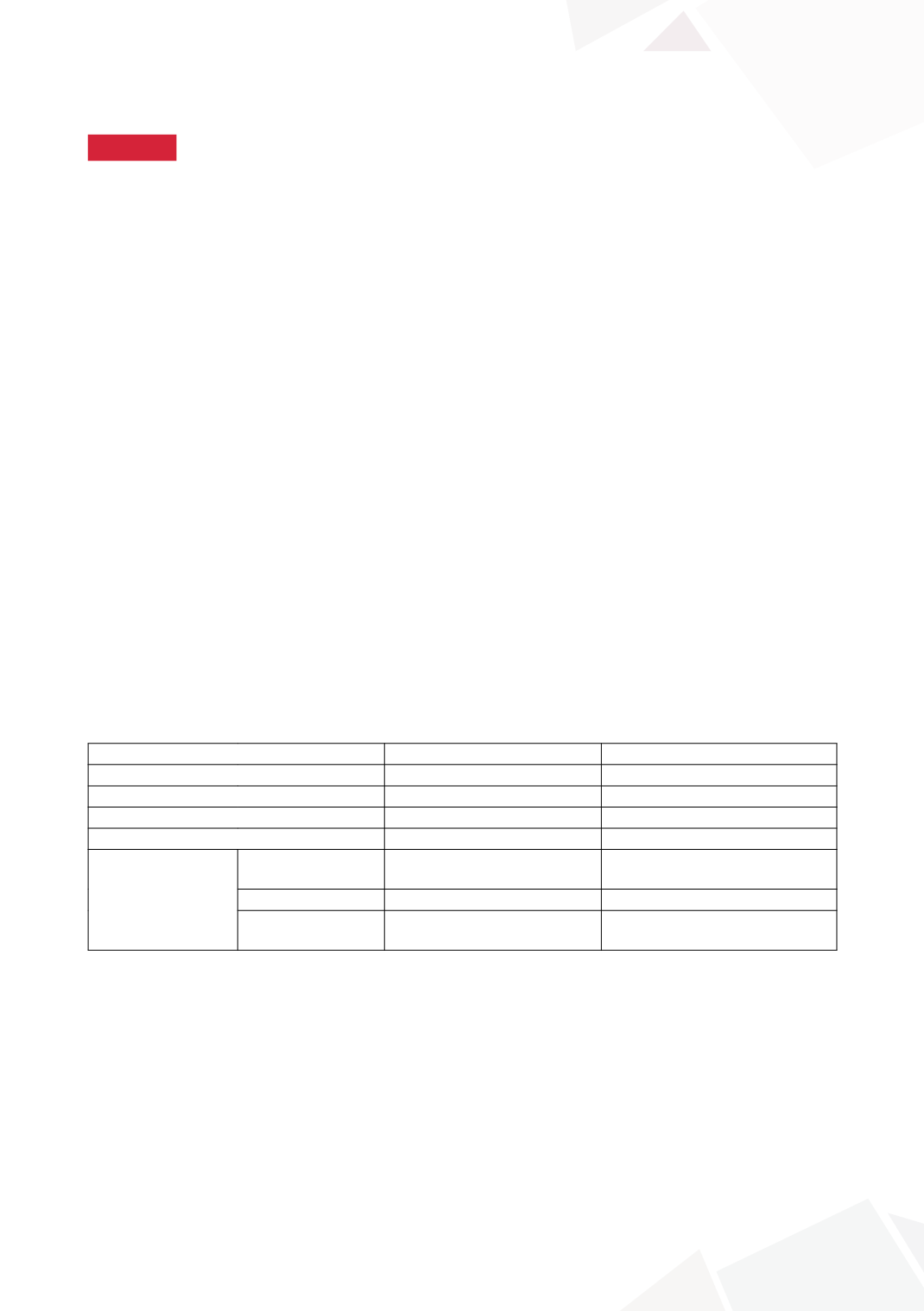
Group
1-Heminephroureterectomy 2–Bladder reconstructive surgery
Number of patients
39
40
Mean age at surgery (years)
3.8(0.8-17.4)
4.7(0.7-16.6)
Mean duration follow-up (years)
9.6(1-13)
3.4(1-7.3)
Further Surgery
11(28%)*
2(5%)*
Risk groups
Dilating reflux grade
3-5
9/15 patients (40%)**
1/18 patients (6%)**
Ureterocele
10/22 patients (45%)***
2/20 patients (10%)***
Both reflux+
ureterocele
5/7 patients (71%)
1/2 patients (50%)
* p=0.006,**p=0.002,***p=0.02
CONCLUSIONS
Bladder reconstructive surgery (BRS) reduces the requirement for further surgery compared to
heminephroureterectomy (HN) in symptomatic patients with a duplex kidney and either dilating
vesicoureteric reflux or ureterocele.
08:47–08:56
Discussion