








 192 / 330
192 / 330

192
28
TH
CONGRESS OF THE ESPU
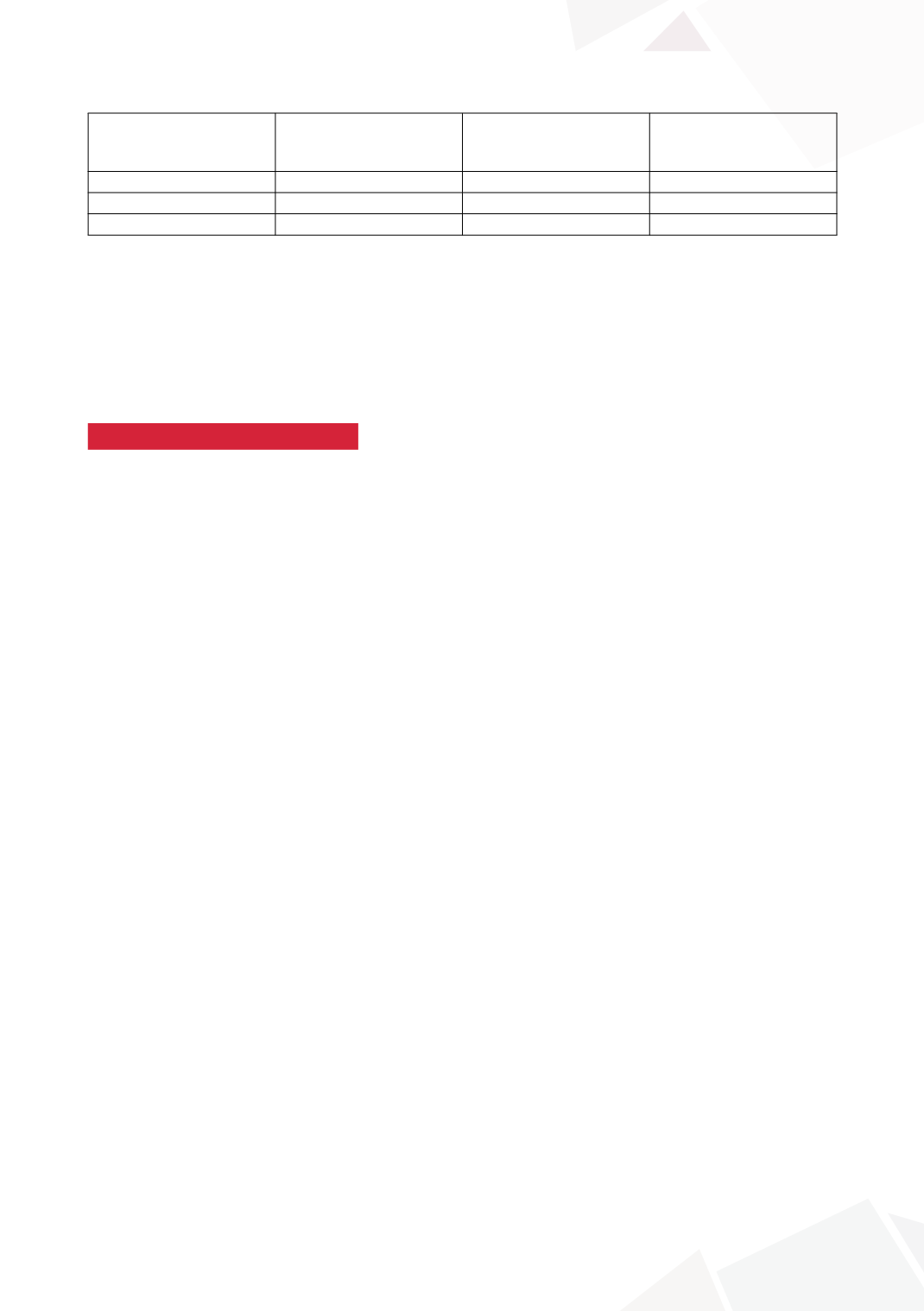
Before ureterocele
excision and ureter(s)
reimplantation
After ureterocele
excision and ureter(s)
reimplantation
statistical relevance
[p-value <0,05]
UTI’s
15/21
3/21
yes
Post-void residual urine 6/21
3/21
no
VUR
4/21
0/21
yes
CONCLUSIONS
1) Ureterocele presenting with complications needs an individualized treatment plan.
2) Patients with recurrent UTI’s, post-void residual urine or persistent VUR after primary endoscopic
treatment or heminephrectomy with ureterocele decompression may still require surgery in the
bladder.
3) Open excision of ureterocele with ureter(s) reimplantation reduces UTI’s and eliminates VUR, but
it doesn’t decrease post-void residual urine.
S17-13 (P without presentation)
IPSILATERAL URETEROURETEROSTOMY: AN ARGUMENT
FOR LOWER TRACT APPROACH IN DUPLEX SYSTEMS
WITH ECTOPIA AND URETEROCELE
Aseem SHUKLA, Trudy KAWAL, Arun SRINIVASAN and David CHU
Children’s Hospital of Philadelphia, Pediatric Urology, Philadelphia, USA
PURPOSE
Upper pole hemi-nephrectomy is traditionally utilized in the management of duplex renal collecting
systems with poorly functioning upper pole moieties with ectopia or ureterocele. Ablative surgery
is, however, associated with a risk of vascular injury to the lower pole moiety and/or ureteral stump
related complications. We hypothesized that ipsilateral upper to lower pole ureteroureterostomy
(IUU) offers a viable and safe alternative even in cases of minimal upper pole function.
MATERIAL AND METHODS
We reviewed all IUU procedures entered into an IRB approved data-registry between 2010 to 2016.
All patients with duplex systems with obstructed upper pole moieties with function less than or
equal to 10% were included in the study. Outcomes assessed were post operative complications
(Clavien-Dindo classification), urinary tract infections (UTI), need for secondary surgery and radio-
logical improvement. IUU was completed by robotic asssited or open approach distal to the pelvic
brim, and ureteral stump was removed.
RESULTS
62 patients underwent ureteroureterostomy (43 robotic 19 open) between 2010 and 2016 at
a median age of 0.92 years. Study cohort comprised of 33 (53.2%) with upper pole moiety func-
tion of less than equal to 10% (median 3%). A total of 22 (66.7%) diagnosed with ectopia, and
11 (33%) with an obstructing ureterocele. 8 of 11 ureteroceles had been incised in infancy and
50% had ureteral reflux present. Robotic assisted IUU was the preferred modality in 23 (70%) and
10 underwent open IUU. Median length of stay was 1 day and median follow up 24 months (range
3 to 72 months). Complications were limited to 2 patients (6%) with febrile urinary tract infection
in the perioperative period. No case proceeded to upper pole nephrectomy, and 96.9% showed
improvement or stable changes on post op imaging.
CONCLUSIONS
This study demonstrates that IUU is a safe, feasible and definitive approach to the management
of children with poorly functioning upper pole moieties in duplex systems. The approach may be
utilized in cases of ureterocele even with upper pole reflux after previous incision.